

Table of contents
Key Orthopedic Medical Billing Updates That Will Shape Your Practice in 2026
As 2026 looms on the horizon, orthopedic practices across the U.S. are bracing for one of the most disruptive years yet in medical billing and compliance. Between fresh CMS prior authorization requirements, sweeping CPT and ICD-10 updates, and shifting interoperability rules, the way you handle orthopedic billing in 2026 will evolve your practice sharply.
Orthopedic Billing Updates: What’s Changing and What You Need to Know
Below, we break down the most consequential medical billing for orthopedic practices and CMS updates, explore how they’ll impact your daily operations, outline what you must do now, and show how aligning with an experienced RCM provider (like us) can ease the transition.
1. CMS Prior Authorization Rule
In September 2025, CMS finalized its Prior Authorization Reform Rule, cutting payer decision windows from 14 days to just 7 calendar days, and mandating electronic prior authorization (ePA) for all Medicare Advantage and commercial payers.
It sounds like a push for efficiency, and in some respects it is, but this shift brings significant compliance pressure. Orthopedic teams must now:
- Submit full clinical documentation with clean-claims at the very first request
- Monitor auto-denials for high-stakes procedures (e.g. total joint arthroplasties)
- Maintain vigorous appeal workflows across the payer portals
A study presented at the AAOS 2025 Annual Meeting found that prior authorization was an ineffective cost-saving measure for patients undergoing primary total hip arthroplasty (THA). “Prior authorization is employed more frequently for various orthopaedic procedures, and it is forcing an added administrative burden on healthcare practices,” said Elizabeth Abe, BS, lead author of the study.
That’s why automating your RCM process or partnering with a prior authorization service provider becomes not a convenience, but a necessity for orthopedic practices aiming to improve workflow efficiency.
Next Steps:
- Conduct a comprehensive documentation audit to ensure all prior authorization requests include full clinical data at submission.
- Integrate or upgrade electronic prior authorization (ePA) tools in your EHR or RCM platform to meet CMS’s digital mandate.
- Track and analyze denial trends, especially for high-volume orthopedic procedures like total joint arthroplasties, to identify recurring issues early.
- Build a centralized appeal and tracking workflow that links payer portals, status updates, and staff responsibilities.
- Evaluate automation or outsourcing partnerships for prior authorization management to reduce turnaround time and compliance burden.
- Partner with BillingParadise to automate prior authorization tasks, from data gathering to submission, and cut approval times by up to 40%.
2. CMS WISeR Model Implementation
Beginning January 1, 2026, the CMS will roll out the WISeR (Wasteful and Inappropriate Service Reduction) model in six states: New Jersey, Ohio, Oklahoma, Texas, Arizona, and Washington. This model avoids overuse in Medicare by increasing oversight on procedures routinely performed in orthopedic practices.
What this means for your orthopedic practice?
- You may face prepayment review or required prior authorization for services CMS flags as overused or high-risk, including epidural steroid injections, cervical fusion, and knee arthroscopic debridement. In total, 17 service categories will be under scrutiny.
- Third-party review organizations, using AI tools and clinician input, can flag or deny claims that don’t clearly meet clinical guidelines. Since they may earn a share of Medicare savings when unnecessary services are reduced, they have a strong reason to challenge your claims.
- The WISeR program runs from 2026 through 2031, and while CMS has included some safeguards, like excluding inpatient-only and emergency services, you will still need to stay on top of things. If your prior authorization approval rate remains above 90%, you have the chance to earn “gold card” status, leading to fewer prior auth hassles and less paperwork.
Medicare accounts for nearly one quarter of US health care spending ($1.03 trillion dollars in 2023) making it an important area for identifying and reducing waste.
How WISeR implementation will impact your orthopedic billing process?
- You’ll be handling a lot more prior auths: The volume will be going up, and that means more time spent just getting approvals.
- Expect more peer-to-peer review calls: Providers may find themselves tied up on the phone, defending medically necessary care.
- Delays and denials are more likely: Even clean claims could face pushback, which slows down your revenue cycle.
- You will need to put extra effort into appeals and documentation: Stronger paperwork and tighter processes will be essential to keep claims moving forward.
There’s no time like the present to audit workflows, train staff on flagged services, and set up pre-bill checks, all to avoid revenue leakage in 2026.
Next Steps:
- Review your services and flag procedures on CMS’s “overuse” or “high-risk” list, update documentation templates to give more importance to necessary services.
- Train your physicians and medical coders on the 17 scrutinized service categories and ensure you clearly record the clinical justifications.
- Establish pre-bill audits for flagged procedures to identify potential compliance or documentation gaps before submitting the claim to Medicare.
- Monitor your prior authorization approval rates: Aim for 90%+ to qualify for gold-card status and reduce your administrative burden.
- Enhance peer-to-peer and appeal readiness by creating the quick-response protocols for denied or challenged claims.
- Leverage AI-driven claim validation tools or third-party review solutions to stay aligned with CMS rules for orthopedic practices.
- Our experts can help your orthopedic team strengthen your workflow and increase coding accuracy by reducing exposure under WISeR’s AI-based review system.
3. CMS’s Episode-based Alternative Payment Model: TEAM
If your orthopedic practice is tied to a hospital, buckle up: starting January 1, 2026, CMS is mandating a new payment model, TEAM (Transforming Episode Accountability Model). And yes, mandatory means no opt-out.
This shift will fundamentally alter how your services are billed, reimbursed, and scrutinized.
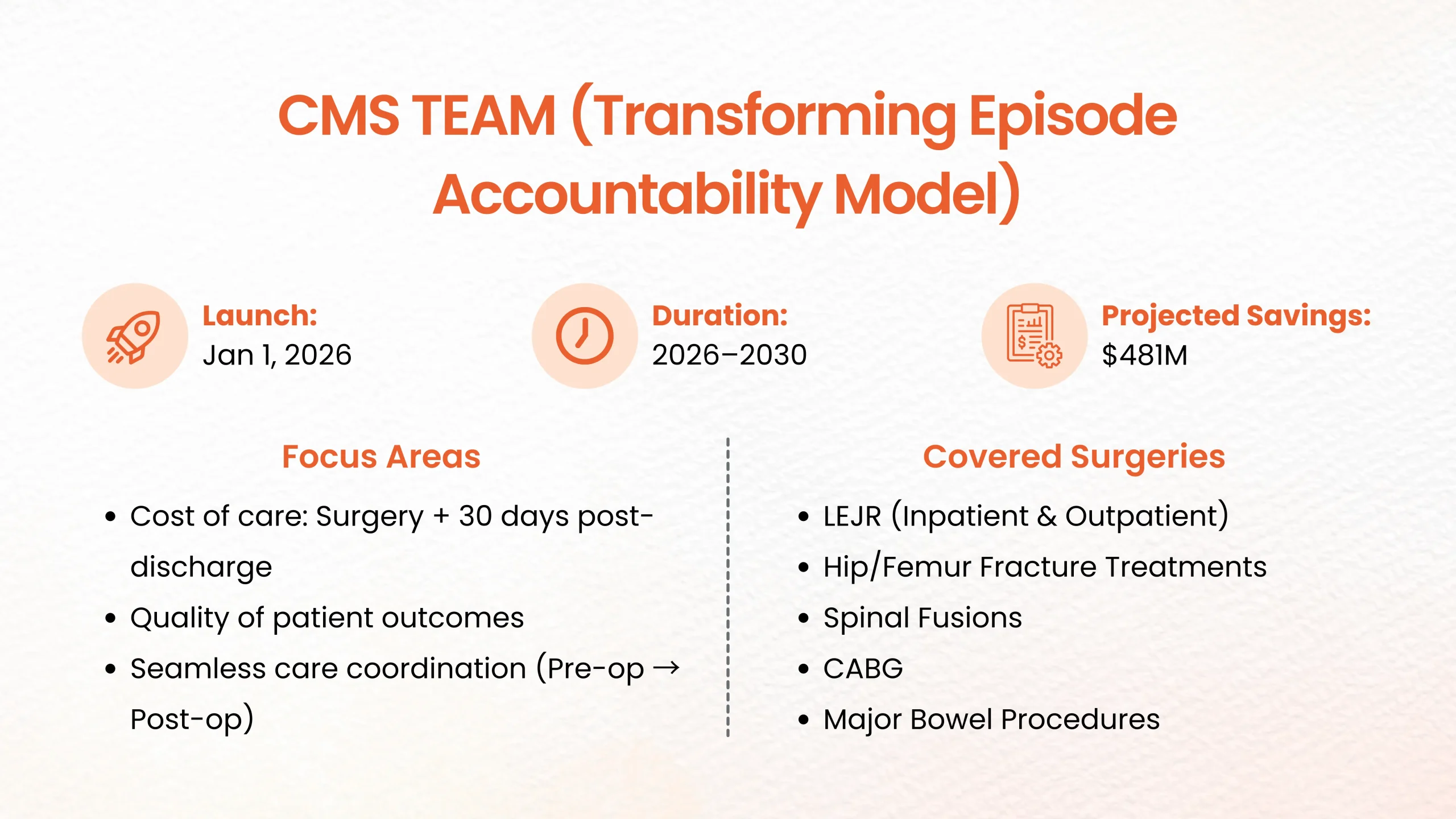
What is the CMS TEAM?
TEAM is an episode-based payment structure that holds hospitals (and affiliated providers) accountable for:
- The cost of care during the surgery plus 30 days post-discharge
- Quality of patient outcomes
- Seamless coordination of care from pre-op through follow-up
The scope of the CMS TEAM model covers five major surgeries, including joint replacements and spinal fusions. Orthopedic surgeries (joint replacements, spine procedures) are high-cost, high-volume, and almost certain to fall within TEAM’s five surgical episodes.
While hospitals carry the risk, orthopedic practices play a significant role in influencing both cost and quality, making their performance crucial for success.
Should the hospital overshoot the budget or fall short on metrics, penalties loom, and your performance will factor into those outcomes.
Highlights to note:
- Launch: January 1, 2026
- Duration: 5 years (2026–2030)
- CMS’s projected savings: $481 million
- Stakeholders: Hospitals, orthopedic surgeons, post-acute care providers
- Coverage: 5 major surgical episodes (Lower Extremity Joint Replacements (LEJR) (inpatient & outpatient), Hip/femur Fracture Treatments, Spinal Fusions, Coronary Artery Bypass Graft (CABG), Major Bowel Procedures
How reimbursement will work?
For each episode, CMS will set a target bundled payment. If the hospital (and its network of providers) stays under budget and meets quality benchmarks, there’s upside. If not, they may owe back a portion of the payment.
That means your protocol efficiency, discharge planning, and follow-up care influence not only patient outcomes, but your hospital’s bottom line.
You’ll need refined billing workflows, rigorous documentation, and seamless data sharing with your hospital partners.
What This Means for Orthopedic Practices?
- Your documentation needs to be airtight. Every little detail counts when payments and audits are on the line.
- Teamwork isn’t optional anymore. You’ve got to stay in sync with hospital staff and post-acute care partners if you want things to run smoothly.
- Don’t treat follow-up and quality data as an afterthought. What happens after surgery can hit your payments directly.
- Expect more eyes on your work. If you let documentation slide, audits and denials are just around the corner.
What To Do Next?
- Start by mapping out your key orthopedic procedures, think joint replacements, spine surgeries, so you know which ones fall under TEAM’s bundled episodes.
- Loop in your hospital partners early. Work together to tighten up documentation, discharge planning, and post-acute workflows.
- Double-check your billing and documentation. Make sure your coding, cost data, and quality metrics all line up.
- Set up shared dashboards or data exchanges so everyone on your care teams can see cost, outcomes, and quality measures in real time.
- Bring your staff and surgeons up to speed on what TEAM means for your bottom line. They need to understand how documentation, patient outcomes, and follow-up tie straight into reimbursement.
- Try running internal simulations or mock episodes. It’s the best way to spot inefficiencies or gaps in care coordination that could cost you when TEAM starts.
And if you want a smoother transition, consider working with revenue cycle experts like BillingParadise. We handle everything from episode cost analytics to optimizing your documentation and forecasting revenue. Let’s make sure you’re ready.


4. 2026 CPT Code Updates: What Ortho Practices Need to Know?
Big changes are coming to CPT codes starting January 1, 2026. The AMA is rolling out 288 new codes, deleting 84, and revising 46 — and a lot of these hit orthopedic billing right where it counts.
Some standout additions: you’ll see new codes for osteotomy procedures that use externally controlled intramedullary lengthening devices, and for repairing vertebral annular defects with bone-anchored closure systems.
If your templates, workflows, or documentation don’t keep up, you’re looking at denials, payment delays, or even audits. So, don’t leave this to chance. Get your team on the upcoming manual, refresh your coding resources, and make sure everyone — especially those working with high-volume procedures — is ready.
What should you do now? Start talking to your payers, update your coding tech, and double-check provider documentation. The goal: smooth revenue, no surprises when these changes hit.
5. Medicare Physician Fee Schedule (PFS) 2026
For 2026, CMS is putting more focus on Remote Patient Monitoring (RPM) and Remote Therapeutic Monitoring (RTM). If you run an ortho practice, there’s a real opening here, as long as you stay ahead of the curve.
Here’s what matters: CMS is letting RPM/RTM services continue under “general supervision” when billed “incident to.” In plain English, non-physician staff like care coordinators or health coaches can handle RPM tasks without the doctor being in the room.
Two new orthopedics CPT codes are on the table:
- A “2-Day” Device Code (99XX4) pays for giving a patient an RPM device used between 2 and 15 days during a 30-day period (instead of the old 16+ day rule). It pays the same as code 99454.
- A “10-Minute” Treatment Time Code (99XX5) covers 10–20 minutes of RPM management and pays half what 99457 does. So, you can bill for shorter but still meaningful check-ins.
Importantly, CMS isn’t cutting rates for the current 99457 or 99458 codes, so those stay valuable heading into 2026.
With these updates, it’s going to get easier to stay compliant and bill for RPM. For ortho practices, that means more monthly reimbursement, better patient tracking, and improved outcomes, all without turning your workflows upside down.
If you’re not using RPM yet, now’s the time. Set up good protocols, train your people, and build RPM into your daily operations. That way, your ortho team can start tapping into this revenue stream and line up with CMS’s push for value-based care.
6. 2026 ICD-10-CM Coding Updates
On October 1, 2025, the new ICD-10-CM update lands, bringing 487 new diagnosis codes, 38 revisions, and 28 deletions across several chapters.
Here’s what should be on your radar:
- Multiple anatomical sites: If a condition affects more than one site, follow the chapter’s specific rules. If there aren’t any, code each site separately. If the note just says “multiple sites,” use the “multiple sites” code.
- Type 2 diabetes in remission (E11.A): Make sure the provider’s note clearly says “in remission.” Don’t use this code for “resolved” or “history of” diabetes.
- HIV coding: The rules for sequencing and when to use B20, Z21, and related codes in cases with other conditions are now clearer.
- For ortho: The musculoskeletal chapter now expects more detail, especially with multi-site conditions. Documentation needs to be spot-on.
Last year’s update already added a bunch of new codes for musculoskeletal injuries and implant failures.
The 2026 changes make it even more important that your surgical and diagnosis codes really match up. But this only works if your coders and clinical teams are fully on board before the new rules kick in.
What should you do?
- Update your code libraries and software.
- Train your coders and clinical staff on the new multi-site coding rules, especially for cases involving more than one joint or area.
- Push for precise documentation, especially with terms like “in remission,” “multiple sites,” or for HIV.
- Expect audits or requests for clarification if your claims don’t match the new standards.
Next steps:
- Take a look at your most common ortho diagnoses now.
- Work with your coding and clinical teams to spot possible problem areas, like multi-site cases.
- Update your audit processes, query templates, and documentation protocols so your revenue cycle keeps running without hiccups.
7. Expanded Medicare Post-Payment Audits
In May 2025, CMS quietly dropped news of its biggest audit expansion in a decade, aimed straight at Medicare Advantage (MA) plans. They’re planning to boost their coder-auditor team from about 40 people to nearly 2,000 by September 1, 2025, all powered by new AI audit tools.
Get ready, review activity is about to speed up in a big way. Instead of CMS looking at around 35 records per health plan each year, they’ll start checking anywhere from 35 to 200, all depending on the plan size.
For orthopedic practices, this isn’t just background noise. It’s more like an alarm blaring in your face. Post-payment audit requests are landing faster, deadlines keep shrinking, and if you miss something, you could be staring down some serious financial trouble.
Here’s what you’re up against when it comes to audits:
- CERT (Comprehensive Error Rate Testing): After claims are paid, CMS reviews them to see if they got it right. Medical necessity, documentation, or coding errors are usually what trip people up.
- RADV (Risk Adjustment Data Validation): These audits zero in on Medicare Advantage payments. CMS is catching up on audits from 2018 through 2024, so don’t be surprised if they pull really old records.
- RAC (Recovery Audit Contractor): These folks look for things like upcoding, missing documentation, or double billing.
- TPE (Targeted Probe & Educate): If your denial rate is higher than average, you’ll probably go through several rounds of this audit. If you tighten things up early, you can avoid falling deeper into the audit rabbit hole.
- UPIC (Unified Program Integrity Contractor): These audits go after fraud, waste, and abuse. They can hit before or after payment, and there’s real legal risk here.
And it’s not just Medicare. You’ll see state Medicaid and Special Investigative Unit (SIU) audits, too. They usually give you just 30 to 45 days to respond.
Why does all this matter so much for medical coding? Because CMS isn’t just hiring more auditors, they’re changing the whole game. With coders jumping from 40 to 2,000 and audit frequency way up, CMS can now cross-check billing data across years, procedures, and providers with a level of detail we’ve never seen before.
Here’s what that means for your Orthopedic practice:
- You might get hit with requests for records tied to claims you thought were long closed.
- If your documentation doesn’t match up, algorithms can spot those gaps and flag dozens of similar claims.
- Denials can snowball fast. An error in one case could get projected across a whole batch of claims.
Orthopedic practices already juggle tough coding for stuff like joint replacements, arthroscopies, and spine work. Now, there’s more scrutiny and tighter deadlines than ever.
How These Medical Billing Updates Hits Orthopedic Practices
Let’s not sugarcoat it, orthopedic clinics are right in the crosshairs with these new policy changes. High-dollar procedures like joint replacements, arthroscopies, and spine surgeries always draw attention, and now they’re front and center for more audits and tighter prior authorization rules.
Get Ready for More Denials and Paperwork Headaches
You’ll feel this in your day-to-day. Here’s what’s coming:
- More cases need prior authorization, even the routine ones.
- Approval timelines are getting tighter.
- Denials go up fast if you don’t have every bit of evidence—imaging, PT notes, clinical narratives—attached.
- DME claims with tricky modifiers (like ST) get stuck in reimbursement limbo.
- The need for real-time data sharing with payers is bigger than ever, but honestly, most EHRs still lag behind.
Think about it: if your practice handles 1,000 surgeries a year, just a 3% bump in denials means hundreds of claims get delayed. That’s tens of thousands of dollars in limbo, just waiting.
The Financial Domino Effect
Late payments and extra work aren’t just annoying, they drag your bottom line:
- Surgeries sit in approval queues, slowing down cash flow.
- Admin teams spend more time chasing resubmissions and appeals.
- Implants and devices get stuck on shelves until payers say yes.
- Some procedures end up postponed or canceled when documentation falls short.
Prior authorization isn’t just a back-office hassle anymore, it’s everyone’s problem. From schedulers to surgeons, every role now touches billing compliance. If your processes aren’t tight, expect more denials, mounting backlogs, and bigger compliance risks.
We’ve seen this firsthand at BillingParadise. We’ve helped clinics untangle their workflows, connecting scheduling, documentation, and billing, so cases don’t go forward without payer approval. That cuts down on cancellations and speeds up payments.
What You Need to Do Now to Fix Your Billing Workflow
Here’s how to get ahead, stay compliant, and keep your revenue flowing:
1. Get Leadership on Board
Make prior authorization a priority at the top. Pull in your CFO, CIO, orthopedic leads, and RCM directors. Build a team that owns CMS readiness and tracks the right numbers.
2. Redesign Your Front-End Workflow
Move authorization steps up in your process:
- Add PA checks to your scheduling checklist.
- Gather imaging, PT notes, and diagnostics before you book the patient.
- Use EHR templates that capture all CMS-required data.
- Tie scheduling directly to billing so nothing gets booked without the green light.
3. Upgrade Your Tech
- Link your EHR and billing systems to payer APIs for real-time PA status.
- Roll out electronic prior auth (ePA) tools.
- Set up dashboards for instant alerts on approvals, denials, and appeals.
4. Invest in Training and Coding Oversight
- Train your team on upcoming CPT and ICD-10 changes for 2026.
- Keep a central “code change library” everyone can access.
- Audit files every month and keep your appeal templates fresh.
5. Work With a Trusted Medical Billing Partner
Don’t go it alone. Reliable medical billing companies like BillingParadise handle end-to-end prior authorization and revenue cycle management. With automation and payer-specific know-how, they help reduce denials, speed up approvals, and keep your cash flow steady.
6. Track the Right Metrics
Watch these numbers to spot problems early:
- PA submission volume
- Approval versus denial rates
- Turnaround times
- Money stuck in delayed claims
These performance KPIs give you a real sense of where revenue is bottling up and where your workflow needs help.
7. Brace Your Finances
Plan for slowdowns. Set aside reserves for late reimbursements and adjust your OR schedule to deal with authorization lags.
8. Get Ahead With Payers
Reach out to your payer reps now. Nail down the latest criteria, clear up what documentation they expect, and use CMS transparency data to see how response times stack up.
Stay proactive, don’t wait for denials to pile up. That’s how you keep your practice running smoothly, even when the rules keep shifting.
Stay Ahead with BillingParadise: Your Orthopedic Billing Partner
Running an orthopedic practice isn’t easy, compliance rules keep changing, and billing mistakes can cost you real money. That’s where BillingParadise steps in. We don’t just help you keep up; we help you use these challenges to grow.
Here’s how we make a difference:
Prior Authorization Pros: Our specialists know orthopedics inside out. They handle every step—submissions, paperwork, follow-ups—so you don’t have to chase after approvals.
Expert Coding: Certified coders stay on top of every CPT and ICD-10 update. They catch errors before claims go out, so you see fewer denials and get paid faster.
Smooth System Integration: We connect your EHR and billing tools with ePA tech. No more data silos or wasted time digging for information.
Denial Management and Appeal Support: Our analytics team digs into every denial, finds the root cause, and builds smart appeals that get results.
Real-Time Analytics: Custom dashboards show you what matters, denials, approvals, payer trends, so you can spot cash flow issues before they become problems.
Ongoing Staff Training: We keep your billing and clinical teams sharp with practical training built around orthopedic requirements.
Results That Matter: We work for your bottom line, faster approvals, fewer denials, stronger cash flow. And we back it up with clear, transparent SLAs.
Is Your Orthopedic Practice Ready for 2026 Billing Compliance?
Big changes are coming in 2026. The new billing rules aren’t just tweaks, they’re a wake-up call. CMS is tightening prior authorization, CPT and ICD-10 code sets are expanding, and real-time data exchange isn’t optional anymore. Every step of your billing process, documenting, coding, billing, getting paid, is about to get tougher.
At BillingParadise, we don’t wait for problems to show up. We build RCM solutions that handle the high-volume, high-complexity world of orthopedics. While others scramble to adjust, you’ll be out front.
Whether it’s speeding up prior authorizations, adapting to new coding rules, or staying compliant with CMS data-sharing mandates, we make it manageable.
Orthopedic billing in 2026 demands precision, speed, and strategy. You don’t have to go it alone.
Let’s get your practice ready for what’s next. Book your free consultation with BillingParadise today.





{kind=link}
{kind=link}